Dr. Dawn Goddard Eckrich Strives to Understand and Prevent Intimate Partner Violence in the Caribbean and US
Dr. Dawn Goddard-Eckrich, Associate Director of the Social Intervention Group and Associate Research Scientist at Columbia School of Social Work, uses her background in implementation science and behavioral intervention research to address important social and behavioral issues, with a particular focus on gender-based violence (GBV) and intimate partner violence (IPV). A native of Trinidad and Tobago, she’s particularly attuned to the high rates of domestic violence and IPV in the Caribbean, where nearly 40% of women experience IPV, a rate 21% higher than the global average. Her work also includes Black women in the United States, another group of women that experience IPV at a disproportionately high rate.
In a forthcoming paper, she and her co-authors map out the gaps in our current understanding of IPV in the Caribbean and Caribbean diaspora. Another of Dr. Goddard-Eckrich’s recent papers, “Patterns of intimate partner violence among black women in community supervision programs who use drugs: a latent class analysis,” found that belonging to a minoritized identity group, such as women who have sex with women, was associated with higher rates of IPV.
What do the findings from these papers suggest are the most important issues to tackle when addressing IPV and GBV?
The research points to two critical areas: the pervasive stigma around intimate partner violence and individual behaviors that perpetuate violence. We need rigorous research into stigma and how it operates at multiple levels including how it prevents survivors from seeking help, silences conversations about violence, and allows harmful patterns to continue unchallenged. We also need to invest in evidence-based behavior change interventions. Without addressing both the social attitudes that enable violence and the individual behaviors that perpetuate it, interventions will fall short.
As you look at IPV and GBV in multiple countries and cultural contexts, what are the patterns you see recurring? What about surprising differences?
One of the most troubling patterns I see recurring across contexts is the inadequate response from institutions that should be protecting survivors, particularly law enforcement and government agencies. When survivors can't rely on these systems for protection or justice, it perpetuates cycles of violence.
Perhaps even more concerning is the public desensitization to this violence. When you read comments on news stories about domestic violence incidents, you see people becoming almost numb to the tragedy, and there's an alarming amount of victim blaming. People may not even realize they're engaging in it. Responses like "Why didn't she just leave him?" or "What did she do to provoke him?" reflect deeply ingrained attitudes that shift responsibility away from perpetrators. This victim blaming, whether intentional or not, creates additional barriers for survivors and reinforces the social conditions that allow violence to continue.
How does this deepened understanding of what increases the risk of experiencing intimate partner violence contribute to developing tools and interventions to prevent IPV?
Understanding risk factors allows us to design interventions that address root causes rather than just responding to symptoms. For instance, we can recognize the role of institutional failure, like inadequate police response or lack of government support, which tells us we need system-level interventions, not just individual-focused programs. Similarly, understanding how victim blaming and desensitization operate in communities helps us design public education and awareness campaigns that actively challenge these narratives. When we know that social acceptance of violence is a key risk factor, we can create community-based interventions that shift norms and attitudes.
What is community-based participatory research? What role does it play in understanding and preventing IPV and GBV?
Community-based participatory research (CBPR) is an approach that treats community members as equal partners in the research process, rather than simply as subjects of study. Instead of researchers coming in from outside, extracting data, and leaving, Similar to what we did with the Healing Communities Study to address the opioid epidemic, CBPR involves community members in every stage, from identifying research questions to designing studies, collecting data, interpreting findings, and implementing solutions.
This approach is particularly important for IPV and GBV research because these issues are deeply embedded in community contexts, power structures, and cultural norms. Community members have lived expertise that academic researchers may not have. They understand the nuances of local dynamics, know what barriers exist, and can identify what interventions might actually work in their specific community. CBPR also builds trust, which is essential when researching sensitive issues like intimate partner violence. When communities are genuine partners in the research, they're more invested in the outcomes, and the interventions that emerge are more likely to be culturally appropriate, sustainable, and effective.
Your work references the importance of tailoring interventions to the cultural context they'll be used in. How does that work? How might an intervention look different when it's designed for, say, women under community supervision in the US versus women in the Caribbean?
Cultural tailoring means recognizing that context shapes everything from how violence is understood and talked about within that community to what resources are available to what kinds of interventions will be accepted and effective.
For women under community supervision in the US, an intervention might need to navigate the criminal justice system, work within the constraints of supervision requirements, and address the intersection of IPV with substance use disorders, housing instability, and the trauma of incarceration. These women may be dealing with mandated reporting requirements, concerns about losing custody of children, or fear of returning to jail. An effective intervention might involve coordination with probation officers, trauma-informed approaches that recognize how the justice system itself can be re-traumatizing, and practical support like housing assistance or legal advocacy.
In the Caribbean context, an intervention may need to account for different cultural and structural factors such as a stronger influence from religious institutions (Hindu, Muslim, or Christian), different family structures and expectations, more limited formal support services, and different attitudes toward law enforcement. Extended family may play a larger role, and there might be more emphasis on community-based support rather than institutional services, and interventions might need to work through trusted community organizations or churches rather than governmental or legal systems.
Additionally, the healthcare system in Trinidad and Tobago and across the Caribbean needs significant improvement to provide the infrastructure necessary for IPV interventions to be truly effective. Without accessible, well-resourced healthcare facilities, trained mental health professionals, and providers educated to screen for and respond to intimate partner violence, even the most culturally tailored interventions will struggle to support survivors or prevent future violence.
In your work, you note the role of heteropatriarchy and masculine identities built around aggression in IPV and GBV. How do you design interventions that address that side of this issue?
You can't address intimate partner violence without addressing the root causes, which means working directly with men and confronting the systems and institutions that perpetuate harmful gender norms. Effective interventions need to include men, not just as perpetrators to be punished, but as people who can change and who can become part of the solution.
This means designing programs that engage men in examining how traditional masculinity has been constructed around dominance, aggression, and control, and offering alternative models of healthy masculinity. But individual-level work isn't enough. We also need to work with churches and other religious institutions that often play powerful roles in reinforcing traditional gender roles and family dynamics. We need to engage schools, workplaces, and community organizations that transmit messages about what it means to be a man. These institutions can either perpetuate violence by supporting existing norms or become active participants in changing them. Transforming gender norms requires addressing both individual attitudes and the social institutions that shape and reinforce those attitudes across generations.
What do you hope to see in the next stages of research on IPV and GBV in the Caribbean? What about in the US?
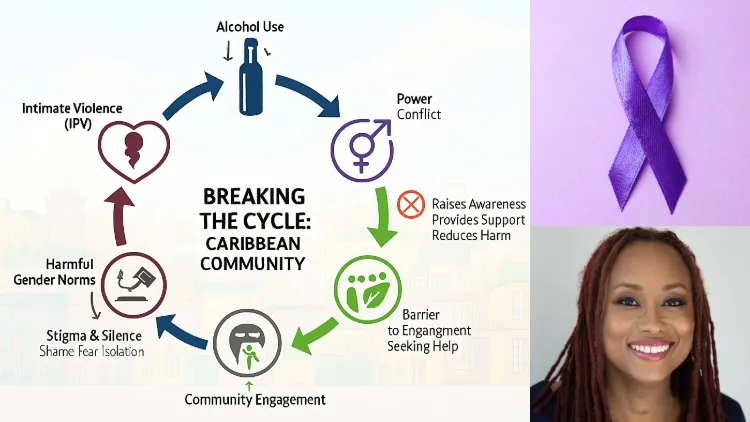
In the Caribbean, I would like to see a community-engaged framework that brings together coalitions across sectors including health care, law enforcement, education, faith communities, and survivor advocates who are all working together with shared goals. Some of this work is already being done by local groups and the UN Spotlight Initiative. We need an extensive communications campaign that reaches people where they are and challenges the normalization of violence. But more than that, we need to really dig deep to understand the root causes. That includes examining the role of alcohol and substance use, which often intersects with violence but isn't always adequately addressed. We need research that doesn't just document the problem but actively works with communities to develop and test locally-driven solutions.
In the US, I'm currently working on the WINGS+++ study in Orange County, New York, and I'm hoping to take some of these mixed methods approaches that combine quantitative data with qualitative community insights and Group Model Building and apply them to work in the Caribbean region. I have incredible partners in Trinidad and Tobago, many of whom are my coauthors on a forthcoming paper, who have been doing this critical work for years, and I recently applied for a grant to do some work in in Grenada. The goal is to develop interventions that are culturally responsive while building on evidence-based practices.
Globally, we need multi-level approaches that work simultaneously on individual attitudes, relationship dynamics, community norms, and institutional responses. This includes education programs that start young, teaching healthy relationship skills and challenging gender stereotypes before harmful patterns are established. It includes bystander intervention training that empowers community members to recognize warning signs and safely intervene. And critically, it includes structural interventions that bring about policy changes, improved law enforcement response, economic support for survivors, and holding institutions accountable for their role in either enabling or preventing violence. No single tool is enough as prevention requires sustained effort across all these levels.
Has anything you've learned from this research changed how you approach anything in your daily life?
This research has made me much more attuned to the subtle ways that violence-supporting attitudes show up in everyday conversation like the casual victim blaming, the jokes that normalize controlling behavior, the ways we talk about relationships that reinforce harmful gender dynamics. I find myself more likely to speak up when I hear/see these things, even when it's uncomfortable. I am the person responding to people in the comments. The research has shown me that prevention starts with these small, daily interactions where norms are either reinforced or challenged.
What makes you optimistic about the future of this research?
I'm excited about the growing recognition that IPV and GBV are public health priorities that require comprehensive, evidence-based approaches and my colleagues at the University of The West Indies, Institute of Gender Affairs and Development and the School of Social Work. There's increasing understanding that these issues intersect with other critical health and social issues like HIV prevention and PrEP access and awareness, so we need integrated approaches. The partnerships I'm building, particularly with dedicated researchers and advocates who have been doing this work for years, give me hope that we can create sustainable change.
But I'd be dishonest if I didn't acknowledge the frustration. There is so much work to be done, not just with IPV but with addressing the stigma around HIV and PrEP access, but funding remains a constant challenge, especially in the current political and economic climate. It's hard to sustain long-term research and intervention programs when resources are uncertain, so my optimism is tempered by realism. I'm excited about what's possible, but I'm also aware of the significant obstacles we face.